
Ending respiratory infections
Introducing Intercept, a $500M bet to make respiratory infections like colds and flu a thing of the past.



A century ago, waterborne diseases levied similar costs to those posed by respiratory viruses like colds and influenza today: endemic, periodically epidemic, and widely accepted as an inevitable feature of human life. Then, at the turn of the twentieth century, we decided they didn’t have to be. Pharmaceutical advances and clean water infrastructure made cholera, typhoid, and dysentery rare across much of the world within a matter of decades.
Why haven’t we already seen the same kind of transformation with respiratory viruses? Last August we hosted a symposium at Stripe with ~40 leading scientists, pharma R&D leaders, biotech venture capitalists, and regulatory experts to better understand if this is technically possible and, if so, why it hasn’t happened yet.
We heard two main reasons. First, it’s just technically very challenging: respiratory viruses represent hundreds of distinct, mutating strains across several families. Fortunately, new platform technologies, advances in our understanding of human immunology, biological data sets, and protein design tools mean we have our strongest ever suite of approaches for tackling it.
Second, the development of the broad-spectrum solutions needed to solve the first problem has historically been underfunded, neither a great fit for philanthropic nor commercial funding. While COVID generated a burst of activity around preventing and understanding respiratory infections through an influx of new funding, that hasn’t been sustained.
We believe that with enough focus and funding, these problems are tractable. Intercept is a $500 million philanthropic initiative that will take advantage of these new tools to catalyze the development of two types of products: broad-spectrum preventatives and air cleaning technologies. Together, these technologies can radically reduce the burden of respiratory infections, and can eventually help eliminate them altogether.
Why this matters
Today, we treat respiratory infections like the cold and influenza as a minor nuisance. The evidence increasingly suggests otherwise.
Healthy people spend roughly 15-25 days each year—about 5% of their lives—sick with respiratory infections like the common cold and influenza.1
Common respiratory infections can lead to severe outcomes. In 2021 alone, there were 12.8 billion infections globally, mostly caused by viruses.2 Annually, over 65 million3 4 of these progress to serious lower respiratory disease and account for around 7% of deaths from major causes in the U.S.5 6 7
Respiratory infections raise our risk of serious illness, often years later. While researchers are still early in establishing these connections, it seems plausible that society has meaningfully underestimated the significance of seemingly benign infections on short and long-term health, e.g.:
9.8x asthma risk by age 6 if infected with HRV between birth and age 3 in a high-risk cohort8
6.1x heart attack risk for 7 days after influenza infection9
4.5-5x dementia risk after severe influenza10
2.6-4.1x Alzheimer’s risk after severe influenza and pneumonia11
2.2-3x schizophrenia potential risk for infant if mother is infected by influenza during pregnancy12 13
1.3x risk of heart failure after RSV infection compared to influenza14
Routine respiratory illness imposes a massive, persistent economic burden, driving 1–1.5% annual productivity losses—roughly $600B globally, or ~0.6% of global GDP—in non-pandemic years.15
Emerging evidence suggests that severe prenatal16 17 and early postnatal18 respiratory infections might lead to reduced adult earnings and educational attainment later in life.
Achieving broad protection against respiratory pathogens would meaningfully reduce pandemic risk, serving as a critical first line of defense—alongside air disinfection—against both natural outbreaks and increasingly accessible engineered biological threats.
Two technologies, working together
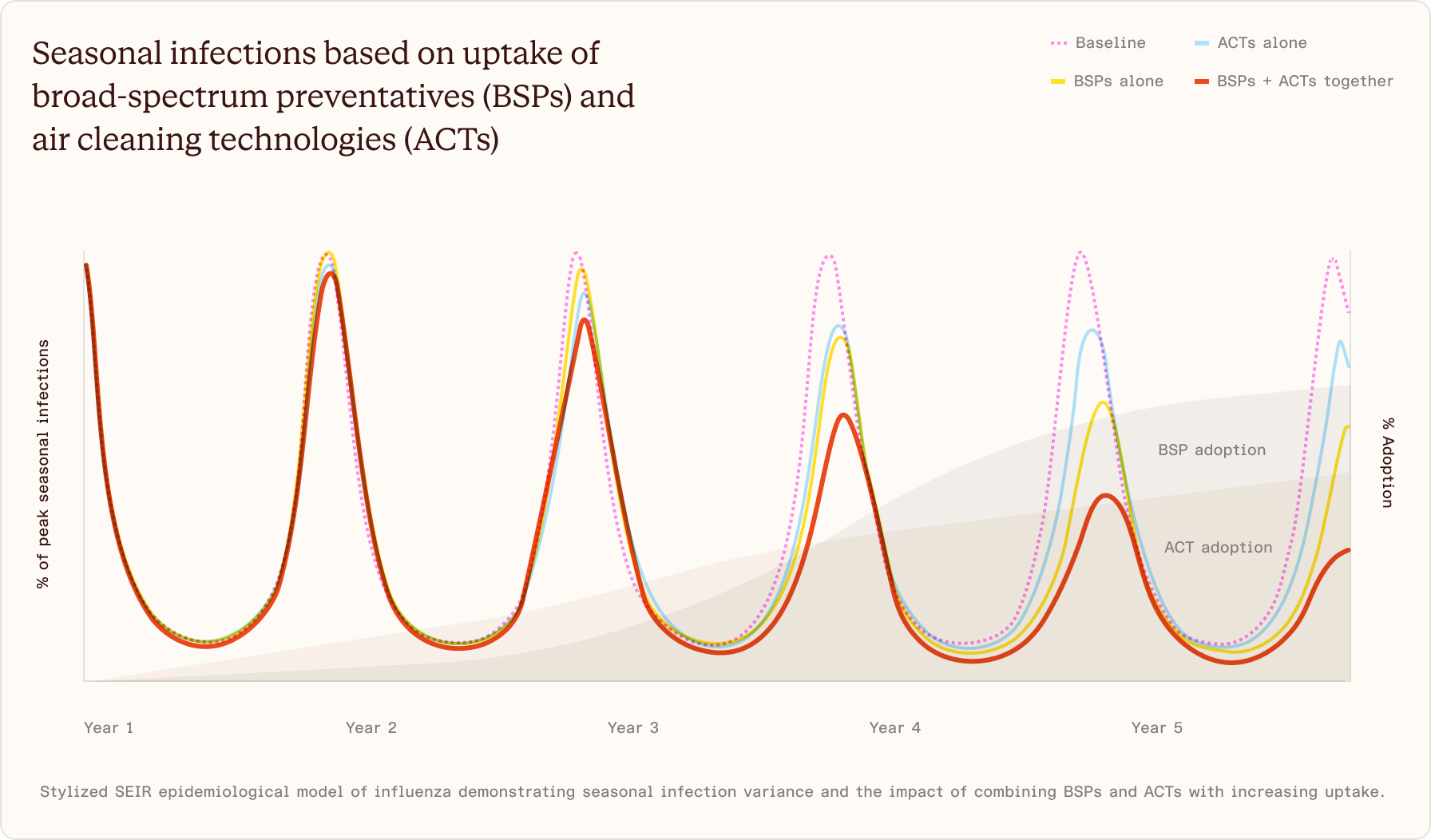
No single technology can accomplish population-level infection reduction across all of these pathogens. A shot or pill that provided >90% protection against >90% of respiratory viruses (we’ll call these broad-spectrum preventatives or BSPs), but achieved ~60% uptake (a realistic ceiling based on existing vaccine uptake), would still fall short of of the population immunity required to dramatically reduce sustained transmissions.
This is because there are so many different kinds of respiratory viruses, many of which are highly contagious. It’s helpful to revisit the concept of R0 from the COVID pandemic: the number of people an infected person will infect in a fully unprotected population. While we can’t change the intrinsic R0 of a given virus, we can reduce any given virus’s effective reproduction number (Re): how infective a virus is in a given environment inclusive of interventions. To eliminate a virus, its Re needs to drop below 1. The vast majority of seasonal respiratory viruses have an R0 between 1 and 3. To eliminate an R3.0 virus, you need roughly 67% of the population to be protected.
So, to get closer to elimination, we also need a way to reduce the virions circulating in high density environments. During COVID the world experimented with various interventions like social distancing and personal protective equipment. But to reduce transmission durably for a large number of common respiratory viruses that are perennially circulating, we need solutions that are convenient and minimally disruptive.
We think the most promising category of products that accomplish these goals are those that remove pathogens from the air, particularly in high-density environments like offices, schools, and public transit. We’ll call these air cleaning technologies (ACTs) like air filtration and far-UVC antimicrobial light.
The uptake required for BSPs or for ACTs to be effective by themselves is extremely high. As a benchmark, commercial fire sprinkler penetration is about 40% in the US. Getting to 100% uptake would be extremely difficult. But when deployed together at realistic levels, BSPs and ACTs could achieve our goals.
Broad-spectrum preventatives (BSPs)
These are products—a shot, a nasal spray, a pill—that defend individuals against rhinoviruses, influenza, coronaviruses, and other respiratory viruses simultaneously. Our goal is to catalyze the development of safe and tolerable preventatives that will prevent more than 75% of symptomatic respiratory infections in as few doses as possible, via easy-to-administer modalities, and that have a credible path to ~60% uptake.19 We will prioritize approaches that are convenient with minimal side effects to support the goals of widespread adoption and uptake. This will be the core technical challenge some of these drug candidates face: they need to find the sweet spot between being too narrow (targeting only one viral strain like most vaccines today) and being too broad (causing unwanted side effects, e.g., via excessive stimulation of the immune system or unwanted off target effects on the host).
Prior to 2020, efforts to develop broad-spectrum preventatives were limited. Then a rapid injection of capital during the pandemic catalyzed a major expansion of research and prototyping. Examples of these include vaccine prototypes designed to elicit broadly neutralizing antibodies across all sarbecoviruses,20 21 small molecule antivirals targeting host proteins with broad antiviral activity,22 engineered interferon-like molecules with broad antiviral activity,23 and siRNA candidates designed for SARS-CoV2.24 Unfortunately, many of these did not progress through clinical development as funding dwindled when effective but strain-specific COVID-19 vaccines became available, but they did provide useful signals on where we might want to focus our efforts.
Adaptive immunity is the arm of the immune system that is targeted to a specific pathogen or parts of a pathogen, leads to long-lasting immunity against re-infection, and is mediated by cellular (T cells) and/or humoral (B cell) responses. Substantial effort and investment has gone into developing “universal vaccines” that aim to elicit broadly neutralizing antibodies for single virus families,25 but these will offer no protection against other respiratory viruses. Emerging evidence suggests that CD8 T cells stationed at the site of infection can stop an infection from establishing after exposure.26 27 New approaches are now being explored to elicit these types of cells in lung tissues to prevent infection by respiratory viruses. Importantly, these platforms must work across diverse populations and account for population-level immune diversity.
Direct-acting antivirals is a wide category of antiviral interventions that lead to direct inhibition of the viral life cycle. While antivirals such as monoclonal antibodies target proteins on the surface of viruses, new nucleic acid degrader28 29 approaches like small-interfering RNA (siRNA) unlock new antiviral targets like viral RNA inside cells that are highly conserved across viruses. Another modality includes broad-spectrum small molecules,30 31 32 33 34 which target conserved virus proteins like RNA polymerase or have broad virucidal activity through membrane disruption. Other modalities include receptor decoys. The main barrier we will aim to address is how to optimally expand (or combine) these platforms to protect across multiple viral families while minimizing unwanted off-target effects.
Innate immunity modulators aim to put the immune system on high alert, but without causing the accompanying cold-like symptoms. New protein design capabilities can engineer interferon, the master regulators of innate immunity, with improved product profiles to generate antiviral responses (interferon-stimulated genes) without the associated inflammatory cytokines. Alternative approaches also include small molecule agonists to activate innate signaling pathways such as cGAS/RIG-I, many of which are actively being evaluated as immunological adjuvants for oncology. Proving that longer-term activation of innate immunity will not lead to chronic immune dysregulation and/or inflammation will be key for this category of preventatives.
Host-directed antivirals work by acting on human targets that viruses depend on to enter or replicate inside cells. The main challenges in this field are identifying host proteins that are shared across multiple viral families and finding ways to target them safely without causing harmful side effects. Anti-PD-L1 antibodies, which have transformed cancer treatment, are among the best-known examples of host-directed therapeutics.
Physical barrier formulations prevent entry of viruses into the body, which is generally achieved through the nasal passage (less frequent transmission can occur through the eyes and mouth). The main challenge this approach will likely face is durability—providing sufficiently long-lasting protection on a reasonable dosing schedule. Options include sprays or gels that coat the nasal lining and enhance natural mucosal protections. Other approaches include exploring high-affinity viral-binding proteins—lectins, mucin domains, neutralizing fragment scaffolds, and sialic acid-presenting glycoproteins—as formulation additives that increase the kinetics and completeness of viral particle capture across the full diversity of respiratory viruses.
The science is promising. What’s holding back progress?
Last August at Stripe we co-hosted a symposium with David Veesler, inviting ~40 leading scientists, pharma R&D leaders, biotech venture capitalists, and regulatory experts. The goal was to understand if it’s technically possible to prevent infections from most common respiratory viruses and, if so, what it’d take to do it.
We surveyed attendees ahead of the symposium. One of our questions was: if this doesn’t happen in the next ~10 years, what will the primary reason be? The number one reason cited was lack of funding, followed by technical feasibility.
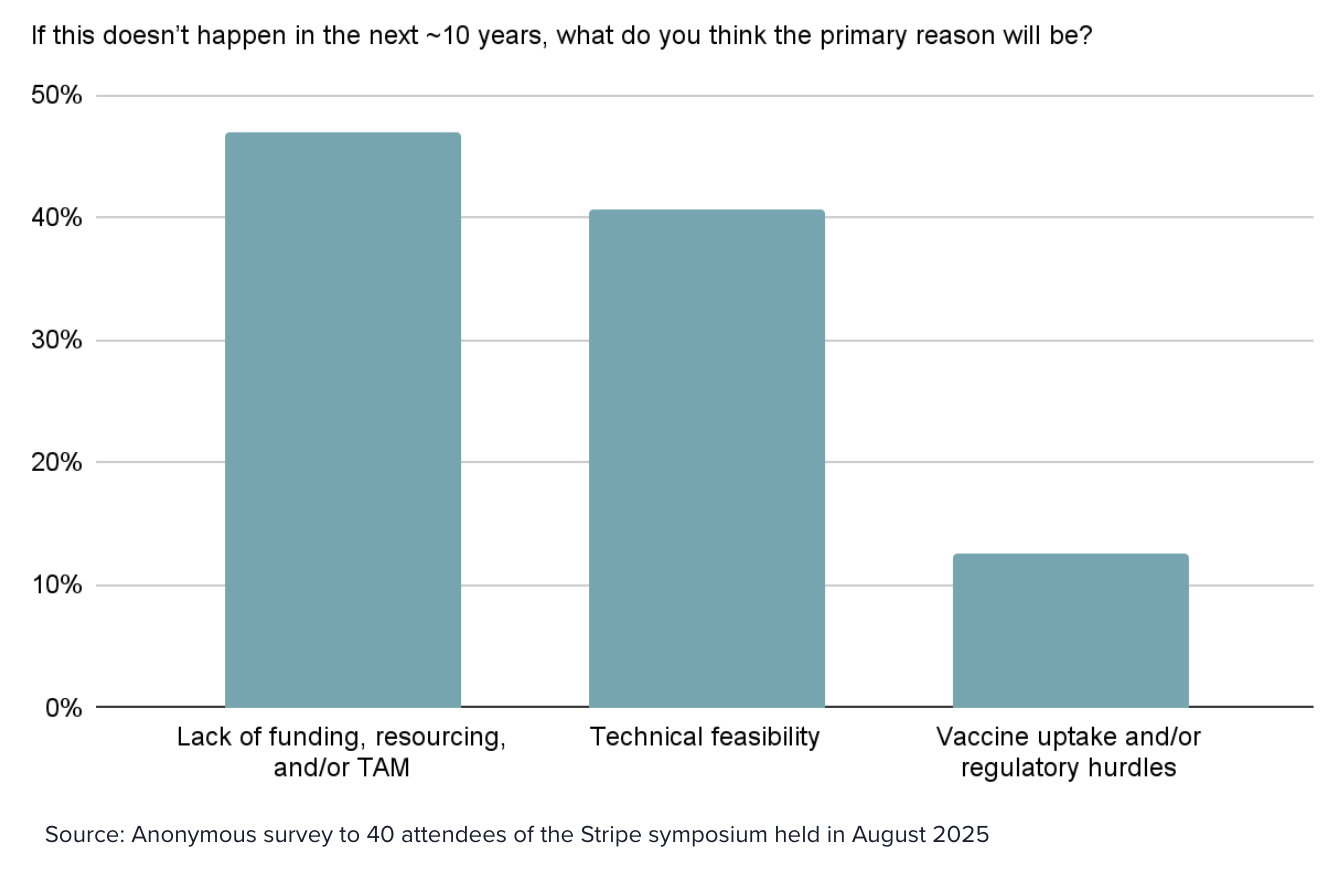
Why hasn’t this field attracted sufficient funding, especially given the enormous societal burden? Common respiratory viruses largely fall through the cracks between government, philanthropic, and commercial funding. In the philanthropic realm, many of these pathogens aren’t a priority for global health, biosecurity or pandemic preparedness funders, who tend to prioritize pathogens that kill large numbers of people, not those that cause an enormous aggregate health and economic burden, but fewer deaths. In the commercial realm, this problem doesn’t attract meaningful biotech or pharma attention because reimbursement tends to reward more severe (or rare) diseases rather than broad population health concerns.
Still, even with sufficient funding, developing a truly broad-spectrum preventative is technically very challenging: respiratory viruses include several different virus families and some have many variants that mutate constantly. Further, the safety bar for developing preventative medicines is appropriately extremely high. If these drugs are to be given to millions of otherwise healthy people, the likelihood they cause harm needs to be extremely low. This means very large and long-lasting clinical trials, which can increase costs and timelines.
Fortunately, developing broad-spectrum preventatives is increasingly tractable for a few reasons. First, modalities developed for other disease areas may enable new categories of broad-spectrum preventatives. Second, new biological data sets and protein design tools may allow us to design new drugs to target conserved features across viruses as well as explore entirely new antiviral strategies.
Our hypothesis is that a well-funded, focused effort significantly improves the odds of creating a broad-spectrum preventative, especially given the tailwinds from recent technical & scientific advances.
Air cleaning technologies (ACTs)
Air cleaning technologies improve indoor air quality by removing or inactivating airborne viruses, just like municipal water infrastructure removes and inactivates pathogens from our drinking water supply. Our goal is to catalyze the uptake of air cleaning technologies that safely reduce infectious aerosols by >75% and have a path to >50% uptake in transmission-relevant indoor spaces at low cost.35
There are several ACTs we’ll focus on initially, each of which layers on top of building ventilation systems that dilute and recycle air. These technologies can often (but not always) be used in combination, and each has unique characteristics that make it more or less well-suited for different types of indoor spaces and use cases.
Air filtration: Products that remove particulate matter and pathogens from the air. Filters can either be placed in the ducts of mechanical ventilation systems to act on recirculated air, or in separate devices placed or mounted in a single room.
Antimicrobial light: A specific wavelength of ultraviolet light (“far-UVC”) that can inactivate pathogens in the air and on surfaces, but does not penetrate human skin or eyes enough to harm dividing cells.
Antimicrobial vapors: Compounds such as triethylene glycol and propylene glycol that can inactivate pathogens in the air and on surfaces, by being drawn into respiratory droplets and inactivating them.
Luckily, most of these technologies we need already exist: far-UVC antimicrobial lights have a growing body of safety and efficacy evidence from the last decade. Air filtration works, but needs to be trialed and scaled to high-transmission spaces. Antimicrobial vapors have been most commonly used in emergency situations, and we need more research to validate whether they could be deployed productively on a continuous basis.
Through interviews with potential customers, public health experts, and suppliers, we’ve consistently heard three pieces of feedback regarding the limited demand for these technologies.
First, while the risk of pathogen spread in indoor air is well-recognized and motivating in pandemic settings, in “peacetime,” decision-makers and the public do not yet view this as an urgent problem. The cumulative impact of our baseline indoor air quality on short-term well-being, long term health outcomes, and economic disruption is simply not widely salient enough to drive investment consideration.
Second, because people can get sick from pathogens in the air in any of the countless places they inhabit throughout the day, it’s challenging to measure the impact of individual ACT deployment projects on infection rates and attendant costs. Studies show that these products are effective at removing pathogens from the air in controlled environments, but there remains a need for more evidence that this works in real-world spaces and that it results in fewer or less severe infections.
Third, while standards for how much clean air is needed in indoor spaces are emerging from organizations such as ASHRAE and the US Green Building Council (which developed LEED certification), it is currently challenging for potential customers to evaluate product quality, safety and effectiveness to achieve those targets. Solving this will require developing a mature ecosystem of installers and evaluators ready to help would-be customers and accepted test standards for product marketing claims, as has been developed for energy efficiency.
These challenges make it difficult to model the return on investment for individual decision-makers and create sustainable, business-case-motivated demand. We believe efforts to make clean air more salient, generate high quality evidence for the efficacy of these technologies, establish clear standards, and invest in high quality suppliers to help customers meet those standards are entirely possible.
Intercept
We’re launching Intercept to catalyze the development and deployment of these technologies. The goal is to radically reduce the global burden of respiratory infections and ultimately eliminate them altogether.
The core of Intercept is a $500M fund that will make grants and investments to de-risk projects and advance them far enough for capital markets to kick in and take them the rest of the way.
With broad-spectrum preventatives, our goal is to advance 2+ products that meet our target product profile through Phase 2, after which the hypothesis is that pharma companies will consider these technically de-risked enough to step in. We’ll pursue a two-track strategy. Track 1 will focus on equity investments to advance available clinical-stage projects to generate phase 2 data in 3-4 years–although these product candidates might not fully meet the target product profile, they will be essential in paving the clinical and regulatory pathways for the next-generation products. Track 2 will be primarily focused on the deployment of grants to support earlier-stage projects that have a higher chance of meeting the target product profile but will likely require longer than 5-7 years to reach commercialization.
With air cleaning technologies, the goal is to generate ‘Phase-3 equivalent’ evidence for these technologies and get those that qualify on a path to widespread adoption. Across the board, we’re not focused on optimizing risk-adjusted returns, but rather on the likelihood of generating approved products with the most efficient form of capital.
To achieve our goal these products not only need to exist, they need to meet the needs of real prospective customers. This is especially true of ACTs. We’ve convened a network of interested buyers who will provide important customer input to ensure the products being developed are the right ones. We’re calling this the Customer Advisory Board. Their involvement helps provide the market signal that has been lacking, as well as iterative feedback as development progresses. Today our Customer Advisory Board includes Stripe, Anthropic, BXP, Kilroy, Jane Street, JP Morgan, Mastercard, Meta and Warby Parker.
Finally, we’ll engage regulators to accelerate the support and obtain the approvals required to bring both sets of products to the market. For BSPs, the hard questions are around how to reduce clinical trial costs and timelines through things like innovative trial design and clinical trial networks, while also charting a path to reimbursement. For ACTs, truly widespread uptake will come from policies that require them in high-transmission environments.
Respiratory infections aren’t inevitable. If we can get these technologies deployed at scale, the change would be profound. Some upsides are measurable: fewer sick days, a healthier economy, a standing line of defence against the next pandemic. Others will be harder to quantify: parenting without the familiar cascade of home and work disruptions, preventing long-term adverse health consequences that can be severe, and winters that don’t hollow out the office.
Developing novel products, navigating complex approvals, and then distributing them at scale is undoubtedly difficult. But it’s more tractable now than it’s ever been. We think we should give it our best shot.
We’re grateful to all of the funders, partners, and advisors who have made this possible.
Our anchor funders include Stripe, Anthropic, Flu Lab, OpenAI Foundation, Patrick and John Collison, a dozen individuals from Jane Street, and Bill Gates through a philanthropic entity. We are further supported by Coefficient Giving. Additional contributions came from Anthropic employees, who gave in an individual capacity.
Intercept will be advised by Moncef Slaoui, Rachel Glennerster, Peter Marks, Keith Klugman, David Veesler, Linsey Marr, Michael Kremer, Jake Swett, Luciana Borio, Vyas Ramanan, Mario Barro, Kabeer Aziz, Zavain Dar, Colin Walsh, Nisha Nanda, Skip Virgin, Craig Shapiro, and Chris Gagliardi.
Symposium attendees: Ali Ellebedy, Anil Patel, Anthony Philippakis, Bali Pulendran, Becca Flitter, Becca Kirby, Brian Wang, Casey Wright, Charlie Petty, Chris Snyder, Darin Edwards, David Kaufman, David Veesler, Davide Corti, Emily Aaronson, Florian Wimmers, Hannah Bebbington, Harry Kleanthous, Jacob Glanville, Jacob Trefethen, Jeremy Ratcliff, Jesse Bloom, Jonah Cool, Josh Morrison, Julie McElrath, Kayvon Modjarrad, Lucy Southworth, Maziar Divangahi, Michael Fischbach, Mihai Netea, Nan Ransohoff, Neil King, Patrick Collison, Patrick Hsu, Peter Kim, Rino Rappuoli, Risako Gen, Saloni Dattani, Skip Virgin, and Trevor Bedford.
Heikkinen T, Järvinen A. “The common cold.” Lancet 2003;361(9351):51–59: https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(03)12162-9/fulltext.
GBD 2021 Upper Respiratory Infections Otitis Media Collaborators, Lancet Infect Dis. 2025 Jan;25(1):36–51.
Mazur et al, Lancet, 2024: https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(24)01716-1/abstract.
Lafond et al, PlosPLoS Med, 2021: https://journals.plos.org/plosmedicine/article?id=10.1371/journal.pmed.1003550.
RSV: Du et al, Int J Infect Dis, 2023.
Jackson et al, Am J Respir Crit Care Med, 2008: https://academic.oup.com/ajrccm/article-abstract/178/7/667/8525947.
Kwong et al, New England Journal of Medicine, 2018: https://www.nejm.org/doi/full/10.1056/NEJMoa1702090.
Levine et al, Neuron, 2023: https://www.sciencedirect.com/science/article/pii/S0896627322011473.
Levine et al, Neuron, 2023: https://www.sciencedirect.com/science/article/pii/S0896627322011473.
Brown et al, JAMA Psychiatry, 2004: https://jamanetwork.com/journals/jamapsychiatry/fullarticle/482040.
Limosen, Acta Psychiatr Scand, 2003: https://onlinelibrary.wiley.com/doi/abs/10.1034/j.1600-0447.2003.00052.x.
Montiel et al, ERS, 2026: https://publications.ersnet.org/content/errev/35/179/250160.
Author’s calculation: 1-1.5% annual workplace productivity lost due to respiratory infections in non-pandemic years from both absenteeism and presenteeism (source: derived from OHE, Employer Costs from Respiratory Infections (2024, Pfizer-funded), and corroborated by Samsudin et al., BMC Infect Dis 2024). Applied to ~$60T in labor income per year globally (the ~52% labor income share from ILO’s World Employment and Social Outlook, Sept 2024, applied to ~$115T global GDP from the IMF’s World Economic Outlook) = ~$600-900B/year.
Schwandt, H (2018), CEPR Discussion Paper No. 12563. CEPR Press, Paris & London: https://cepr.org/publications/dp12563.
Almond, D. (2006). Journal of Political Economy, 114(4), 672–712: https://doi.org/10.1086/507154.
Daysal, N. Meltem and Ding, Hui and Rossin-Slater, Maya and Schwandt, Hannes, IZA Discussion Paper No. 18078: http://dx.doi.org/10.2139/ssrn.5403493.
Re = R0 × (1 - 75% BSP efficacy × 62% BSP uptake) × (1 - 75% ACT efficacy × 50% ACT uptake) = R0 × 0.334, or Re < 1 (i.e., elimination) for viruses with R0 < 3.0
Re is the effective reproduction number, or the actual average number of secondary infections at a given moment, accounting for whatever immunity, interventions, and behavior are currently in place. R0 is the basic reproduction number, or the average number of secondary infections produced by a single infected person in a fully susceptible population, with no interventions in place.
Halfmann et al, eBioMedicine, 2022: https://www.thelancet.com/journals/ebiom/article/PIIS2352-3964(22)00523-0/fulltext
Cohen et al, Science, 2022: https://www.science.org/doi/10.1126/science.abq0839
Elizabeth Walsh, ACS, 2022: https://pubs.acs.org/doi/pdf/10.1021/acscentsci.5c02070
Yen et al, Cell, 2022: https://www.cell.com/cell/fulltext/S0092-8674(22)00247-1
Idris, Molecular Therapy, 2021: https://www.cell.com/molecular-therapy-family/molecular-therapy/fulltext/S1525-0016(21)00256-2
Walls et al, Cell, 2021: https://www.cell.com/cell/fulltext/S0092-8674(21)01062-X
Swadling, et al, Nature, 2021: https://www.nature.com/articles/s41586-021-04186-8
Kalimuddin et al, Nature Microbiology, 2025: https://www.nature.com/articles/s41564-024-01903-7
Hariharan et al, PNAS, 2023: https://www.pnas.org/doi/abs/10.1073/pnas.2219523120
Idris, et al, Molecular Therapy, 2021: https://www.cell.com/molecular-therapy-family/molecular-therapy/fulltext/S1525-0016(21)00256-2
Ezzatpour et al, Science Advances, 2025: https://www.science.org/doi/10.1126/sciadv.ady3554
Mathez et al, Science Advances, 2025: https://www.science.org/doi/10.1126/sciadv.adv9311
Jones et al, Science Advances, 2020: https://www.science.org/doi/10.1126/sciadv.aax9318
Xia et al, Science Advances, 2019: https://www.science.org/doi/10.1126/sciadv.aav4580
Woods et al, bioRxiv, 2025: https://www.biorxiv.org/content/10.1101/2025.01.13.632836v3
Re = R0 × (1 - 75% BSP efficacy × 62% BSP uptake) × (1 - 75% ACT efficacy × 50% ACT uptake) = R0 × 0.334, or Re < 1 (i.e., elimination) for viruses with R0 < 3.0
Re is the effective reproduction number, or the actual average number of secondary infections at a given moment, accounting for whatever immunity, interventions, and behavior are currently in place. R0 is the basic reproduction number, or the average number of secondary infections produced by a single infected person in a fully susceptible population, with no interventions in place.